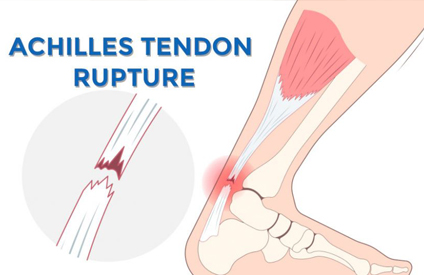
Achilles Tendon Rupture
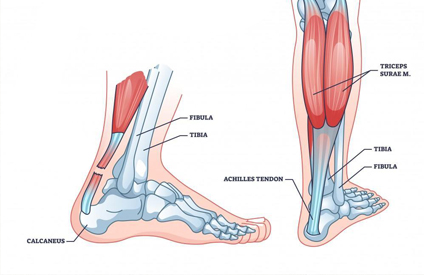
The Achilles tendon (calcaneal tendon) is the largest and strongest tendon in the body, connecting the gastrocnemius and soleus muscles to the calcaneus (heel bone). It’s crucial for walking, running, and jumping. A rupture occurs when the tendon fibers tear completely or partially.
Achilles tendon rupture usually happens during sudden, forceful activities or in tendons weakened by degeneration.
Common Causes:
- Sudden acceleration or push-off movements: Jumping, sprinting, or pivoting (e.g., basketball, soccer, tennis).
- Sudden dorsiflexion of a plantar-flexed foot (landing from a jump).
- Chronic tendinopathy or degeneration: Microtears and reduced blood supply make the tendon more prone to rupture.
- Medication-related weakness:
(a) Long-term corticosteroid use or local injections.
(b) Fluoroquinolone antibiotics (e.g., ciprofloxacin, levofloxacin). - Systemic conditions: Diabetes, rheumatoid arthritis, chronic kidney disease.
- Age: Most common in men aged 30–50 during recreational sports.
Symptoms: Typical signs and symptoms include:
- Sudden, sharp pain in the back of the ankle or calf (“felt like being kicked or shot”).
- Popping or snapping sound at the time of injury.
- Weakness or inability to push off when walking.
- Difficulty standing on tiptoes.
- Visible or palpable gap above the heel (2–6 cm above calcaneus).
- Swelling and bruising around the lower calf and ankle.
Clinical test:
Thompson test (calf squeeze test): When the calf is squeezed, there’s no plantarflexion of the foot → indicates rupture.
Treatment:
Treatment depends on patient age, activity level, and rupture severity.
- A. Conservative (Non-Surgical)
- B. Used for partial tears or less active patients.
- Functional bracing or cast immobilization: Foot in plantarflexion (“toe-pointed down”) for 6–8 weeks.
- Gradual dorsiflexion adjustments as healing progresses.
- Physical therapy: Strengthening, flexibility, and balance training after immobilization.
Surgical Repair
- Complete ruptures.
- Active or athletic patients.
- Re-ruptures or delayed diagnosis.
Procedures
- Open repair: Suturing the torn tendon ends directly.
- Percutaneous repair: Minimally invasive, smaller incisions.
- Augmentation or graft: For chronic or large gaps (using FHL tendon grafts).